ASCO: Treating Lung Cancer After Targeted Therapy–Resistance
By Howard West, MD1 | 2013年6月11日
1Medical Oncologist, Swedish Cancer Institute, Seattle
Interviewed by Anna Azvolinsky, PhD
Cancer Network: Dr. West, non–small-cell lung cancer is becoming increasingly defined by molecular subtypes. Could you go over what the established subtypes are and the available agents that target these?
Dr. West: Well, we are increasingly doing molecular testing on the vast majority of patients with non–small-cell lung cancer. When we talk about molecular testing, we are really focusing this point on patients with non–small-cell lung cancer subtypes, so the approximately 87% or 88% of lung cancer that is non–small-cell. Then, within that group, adenocarcinoma comprises about 60% or so of the patients in the United States, and most of our patients who have an actionable target have an adenocarcinoma, but there are some patients who have the squamous subtype, which is about 20% to 25% of non–small-cell, and they are less commonly found to have an actionable mutation and are a subgroup of patients that we don’t routinely send for molecular testing. There is another small group of patients who don’t fit into the adeno or squamous non–small-cell, and they have a variable probability of having mutations so we still test them. Specifically, the mutations we are looking for are EGFR, or the epidermal growth factor receptor, which is seen in about 10% to 15% of patients in North America and more like 25% to 30% of those in Asia—also ALK rearrangements, which occur in about 4% of patients with non–small-cell and predominantly those with adenocarcinoma. Both of these mutations are more commonly seen in patients with no smoking or minimal smoking history. Finally, there is a mutation called the ROS1 rearrangement that is less common, only about 1% of patients, and these patients seem to respond to the ALK inhibitor drug crizotinib that was approved for patients with the more common ALK rearrangement. So, this testing for ROS1 is not as prevalent yet, not as widely available but is increasingly being tested for, at least by many lung cancer specialists who have found patients who can benefit greatly from these treatments. Because when you do have a driver mutation and the right target, we see a probability of response and depth of response that we just don’t see with chemotherapy.
Cancer Network: So, what is the best time for patients to receive the targeted therapies you mentioned, the EGFR inhibitors and the ALK inhibitors?
Dr. West: In general, there is a consensus that we should be giving these therapies as early as possible, as soon as you know a patient has a mutation that could have a high association with a good response. The treatments that we are talking about in the United States, erlotinib for patients with EGFR mutations or crizotinib for patients with an ALK rearrangement, are oral therapies that are typically better tolerated than chemotherapy, or at least generally very well tolerated. They certainly lend themselves to longitudinal administration because they tend to not have many cumulative side effects. They give a high probability of response in the range of 60% to 75% and a degree of response that we just don’t see with standard chemotherapy. We do tend to favor these being the first therapy that you give if you find that a patient has one of these driver mutations before you start them on systemic therapy. We don’t have complete proof that it is better in terms of overall survival to give these therapies first rather than a maintenance therapy or second-line or later. I think many patients will do just as well if they end up getting these very effective drugs as second-line or later therapy. But, unfortunately, some patients do have unforeseen and catastrophic complications—perhaps leptomeningeal disease, which is involvement of the brain with the cancer that can lead to a rapid decline. Patients can miss that opportunity for treatment that can produce rapid and long-lasting responses, and that is exactly what we want to avoid. So, in general, just about everybody is inclined to give the drugs early on.
Cancer Network: How long do patients generally respond to EGFR inhibitors or crizotinib, and is there a way to predict response length?
Dr. West: There is not a good way to predict this in both EGFR mutation patients and those with an ALK rearrangement. The median duration of response before patients progress is in the range of 8 to 12 months, varying from one patient to another. Typically within a year, but there are a minority of patients who continue to do well for several years at a time, even a few beyond 3 or 4 years. There is a little bit of evidence that is not as consistently reported that patients with a particular mutation in EGFR, called exon 19, have the greatest probability of prolonged response compared with those with another activating mutation on exon 21. But, that is about the only predictive marker we have and even that is not that consistent, so we really can’t say whether someone is likely to respond for a few months or several years to these agents. That said, the degree of response that we see in a patient tends to be correlated with how well they do, so the patients who immediately feel better and whose imaging shows a dramatic response are also often the patients who have the longest responses.
Cancer Network: Most patients’ tumors eventually acquire resistance to the targeted therapies you mentioned. How is resistance typically detected and defined, and what are the issues with defining resistance in the clinic?
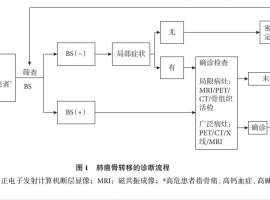
Dr. West: Resistance is typically detected by routine imaging. When we are following someone with lung cancer and we do chest CT scans or sometimes PET-CT every few months, we will generally see a new lesion in the liver, the lungs, or the bone, or a growing lesion that we have been following for a while. If the changes are significant enough, that will be considered progressing disease; it has to do with the dimensions of the tumor. It is important to recognize that small subtle changes, or even a new lesion or two, don’t necessarily lead most experts to want to make a change in therapy. We can see very slow, indolent, and not clinically significant progression of disease long before a patient actually needs to make any change at all. Many patients will go 3 months, 6 months, even a year or longer before they have enough change that the treating physician with a lot of experience concludes that there is an incentive to make a change in treatment—whether that is discontinuing the targeted therapy and making a switch to chemotherapy, or adding chemotherapy and continuing the targeted therapy. There are also some patients who will have new symptoms related to their cancer, whether an area of pain from a bone lesion or new headaches, vision changes that lead to a head MRI and show that someone has a new brain metastases, that are of course clinically significant. But with regards to brain lesions in particular, many experts are really not inclined to discontinue the targeted therapy because brain lesions that arise in this setting don’t necessarily represent resistance to the drug as much as the drug just not being able to get into the central nervous system. Many of these patients can be treated for their brain metastases, with radiation for instance, and continue to do extremely well for months or even years on the ongoing targeted therapy.
Cancer Network: What are the current treatment options for patients who do become resistant to targeted agents? Is it mostly chemotherapy?
Dr. West: Well, there are a growing number of clinical trials, sometimes with novel agents, and certainly these are very appealing options when they are available. Outside of that, we do generally favor chemotherapy. If patients have received first-line targeted therapy, then we generally try to approach treatment with the same chemotherapy options as for someone who is being treated in the first-line setting and who doesn’t have a mutation. Typically, this would be a platinum-based doublet, potentially with bevacizumab(Drug information on bevacizumab), the antiangiogenic agent. Some experts favor continuing the EGFR or ALK inhibitor, and some favor discontinuing it and even potentially restarting it later because we sometimes do see responses or at least prolonged stable disease after rechallenging the patient, even with a drug that they had progressed on earlier because sometimes patients’ tumors can become resensitized to that targeted therapy after a period off of these drugs.
Cancer Network: Lastly, are there any issues with developing resistance to targeted therapies and treatment of patients that we haven’t touched upon yet?
Dr. West: I would say that there is a lot of controversy about whether repeat biopsies should be done in all patients, whether this is a desirable option or whether this should really be bothered with at all. We will sometimes see a change in the histology of the cancer from non–small-cell lung cancer to small-cell lung cancer in somewhere between 3% to 14% of patients who develop resistance. This was actually a very hard to believe finding when it was first reported several years ago, but it has been confirmed by several different studies. You can sometimes see small-cell lung cancer lesions that developed while the patient was on an EGFR inhibitor for months or years, and these patients even have EGFR mutations in non–small-cell lung cancer, so it seems to be an actual transformation. Many of these patients can respond very well to the chemotherapy approaches used routinely for small-cell lung cancer, which is typically a platinum drug with etoposide(Drug information on etoposide) in North America. So, that is one incentive to potentially do a biopsy on a progressing lesion. But, that is also a minority of patients. Outside of that, we really don’t have examples of an actionable result that will lead to a change in treatment based on a biopsy. I don’t consider this a standard of care. That said, I do favor getting tissue whenever possible because this has been the way the field has moved forward to understand the molecular mechanisms underpinning acquired resistance. There have been a growing number of clinical trials with targeted therapies that require tissue. I would say that our biggest advances that we have made in the field in non–small-cell lung cancer have been based on molecular oncology, so the limitation of not having enough tissue is going to limit our understanding and the availability of new therapies. The best thing we can do, even if it is not yet the standard of care, is to get more tissue to try to understand things better.
|
 肺癌脑转移治疗,放疗时机选不对,真
作者:seacat
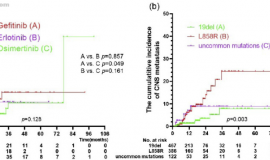
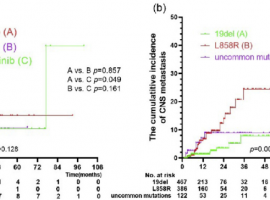
脑部是EGFR突变非小细胞肺癌常见转移部位,虽然第三代EGFR-TKI能显著延
肺癌脑转移治疗,放疗时机选不对,真
作者:seacat
脑部是EGFR突变非小细胞肺癌常见转移部位,虽然第三代EGFR-TKI能显著延
 惋惜 关于一位术后2期肺腺癌病友止步
曾经一起抗癌的老病友很多都陆陆续续地抗癌结束了,如今都各自有了新的生活,当
惋惜 关于一位术后2期肺腺癌病友止步
曾经一起抗癌的老病友很多都陆陆续续地抗癌结束了,如今都各自有了新的生活,当
 无靶点 her2扩增 二线白紫耐药后怎么
家父今年62岁,22年11月份颈部淋巴结穿刺,确诊肺低分化腺癌,分期是TxN3M1,基因检测
无靶点 her2扩增 二线白紫耐药后怎么
家父今年62岁,22年11月份颈部淋巴结穿刺,确诊肺低分化腺癌,分期是TxN3M1,基因检测
 SMARCA4-NSCLC 盲试靶向药有效!!
首先感慨一下今天真的是个好日子。努力了进三个月的治疗终于有了重大进展。
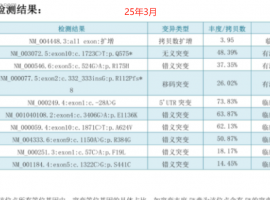
复查结果
SMARCA4-NSCLC 盲试靶向药有效!!
首先感慨一下今天真的是个好日子。努力了进三个月的治疗终于有了重大进展。
复查结果
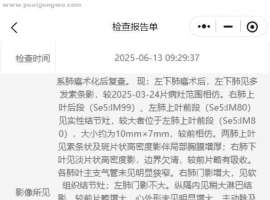 肺腺癌术后一年复查,这是复发转移了
【基本病情:2024年4月底确诊肺癌,五月初手术,术后分期3A期,肺腺癌,淋巴结转移,
肺腺癌术后一年复查,这是复发转移了
【基本病情:2024年4月底确诊肺癌,五月初手术,术后分期3A期,肺腺癌,淋巴结转移,






 显身卡
显身卡