http://www.ncbi.nlm.nih.gov/pubmed/21194487
BMC Cancer. 2011 Jan 1;11:1. doi: 10.1186/1471-2407-11-1.
Clinical responses to EGFR-tyrosine kinase inhibitor retreatment in non-small cell lung cancer patients who benefited from prior effective gefitinib therapy: a retrospective analysis.
Watanabe S, Tanaka J, Ota T, Kondo R, Tanaka H, Kagamu H, Ichikawa K, Koshio J, Baba J, Miyabayashi T, Narita I, Yoshizawa H.
Author information Department of Medicine, Niigata University Medical and Dental Hospital, Niigata City, Japan. satoshimd@yahoo.co.jp
Abstract
BACKGROUND: Gefitinib was the first epidermal growth factor receptor-tyrosine kinase inhibitor (EGFR-TKI) approved for the treatment of advanced non-small cell lung cancer (NSCLC). Few treatment options are available for NSCLC patients who have responded to gefitinib treatment and demonstrated tumor progression. The present study was conducted to evaluate the efficacy and toxicity of the 2(nd) EGFR-TKI administration.
METHODS: We retrospectively analyzed 11 patients who had obtained a partial response (PR) or stable disease (SD) with gefitinib treatment and were re-treated with EGFR-TKI after failure of the initial gefitinib treatment.
RESULTS: Three patients (27%) were treated with gefitinib as the 2(nd) EGFR-TKI, and 8 patients (73%) received erlotinib. Only one patient (9%) showed PR, 7 (64%) achieved SD, and 3 (27%) had progressive disease. The disease control rate was 73% (95% CI, 43% - 91%) and the median progression-free survival was 3.4 months (95% CI, 2 - 5.2). The median overall survival from the beginning of the 2(nd) EGFR-TKI and from diagnosis were 7.3 months (95% CI, 2.7 - 13) and 36.7 months (95% CI, 23.6 - 43.9), respectively. No statistical differences in PFS or OS were observed between gefitinib and erlotinib as the 2(nd) EGFR-TKI (PFS, P = 0.23 and OS, P = 0.052). The toxicities associated with the 2(nd) EGFR-TKI were generally acceptable and comparable to those observed for the initial gefitinib therapy.
|
 肺腺癌术后一年复查,这是复发转移了
【基本病情:2024年4月底确诊肺癌,五月初手术,术后分期3A期,肺腺癌,淋巴结转移,
肺腺癌术后一年复查,这是复发转移了
【基本病情:2024年4月底确诊肺癌,五月初手术,术后分期3A期,肺腺癌,淋巴结转移,
 无靶点 her2扩增 二线白紫耐药后怎么
家父今年62岁,22年11月份颈部淋巴结穿刺,确诊肺低分化腺癌,分期是TxN3M1,基因检测
无靶点 her2扩增 二线白紫耐药后怎么
家父今年62岁,22年11月份颈部淋巴结穿刺,确诊肺低分化腺癌,分期是TxN3M1,基因检测
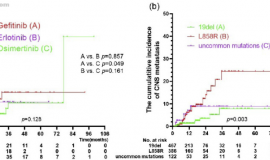
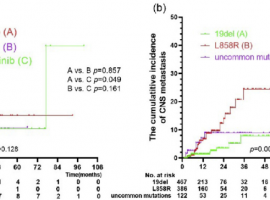 肺癌脑转移治疗,放疗时机选不对,真
作者:seacat
脑部是EGFR突变非小细胞肺癌常见转移部位,虽然第三代EGFR-TKI能显著延
肺癌脑转移治疗,放疗时机选不对,真
作者:seacat
脑部是EGFR突变非小细胞肺癌常见转移部位,虽然第三代EGFR-TKI能显著延
 惋惜 关于一位术后2期肺腺癌病友止步
曾经一起抗癌的老病友很多都陆陆续续地抗癌结束了,如今都各自有了新的生活,当
惋惜 关于一位术后2期肺腺癌病友止步
曾经一起抗癌的老病友很多都陆陆续续地抗癌结束了,如今都各自有了新的生活,当
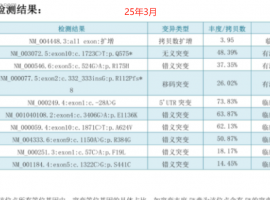
 SMARCA4-NSCLC 盲试靶向药有效!!
首先感慨一下今天真的是个好日子。努力了进三个月的治疗终于有了重大进展。
复查结果
SMARCA4-NSCLC 盲试靶向药有效!!
首先感慨一下今天真的是个好日子。努力了进三个月的治疗终于有了重大进展。
复查结果






 显身卡
显身卡