Erlotinib showed promise as neoadjuvant therapy in patients with epidermal growth factor receptor (EGFR) mutant stage IIIA-N2 non-small-cell lung cancer (NSCLC) who demonstrated good disease control with tolerable toxicity following treatment.
Dr Baohui Han, Pulmonary Department, Shanghai Chest Hospital, Shanghai, China presented findings from a single arm, phase II clinical trial during the New Treatment Avenues Proffered Papers session at the European Lung Cancer Conference, 15 to 18 April 2015 in Geneva, Switzerland. The trial aimed to evaluate efficacy and safety of erlotinib as neoadjuvant treatment in patients with stage IIIA-N2 NSCLC and activating EGFR mutation.
Erlotinib as neoadjuvant treatment in endobronchial ultrasound confirmed stage IIIA-N2 NSCLC patients with EGFR mutation (exon 19 or 21), ESTERN: A prospective, single arm, phase II clinical trial.
© Baohui Han
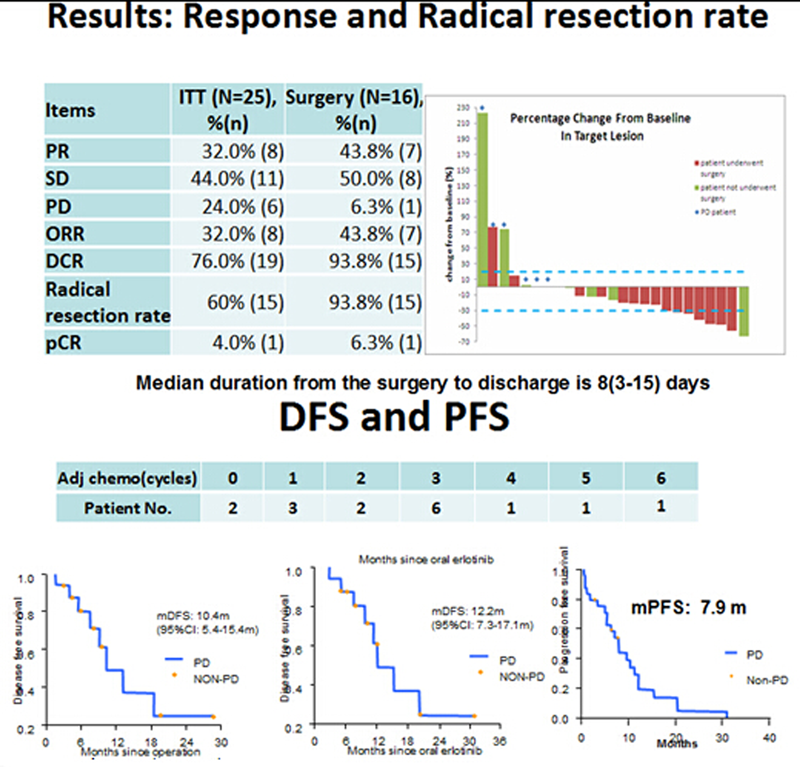
The trial’s primary endpoint was radical resection rate. Secondary endpoints included pathological complete response rate (pCR), objective response rate (ORR), disease free survival (DFS), overall survival (OS), safety profile, and explorative biomarkers.
This study screened 155 patients and subsequently enrolled 44 patients with stage IIIA N2 NSCLC and 25 patients with IIIA N2 NSCLC plus activating EGFR (exon 19 or 21) mutations. All patients had ECOG performance status 1 and had been previously untreated for stage IIIA-N2 NSCLC, that was confirmed by endobronchial ultrasound.
During the 56-day neoadjuvant phase, all patients received erlotinib 150 mg orally per day. Only patients that showed benefit from erlotinib and were evaluated as resectable following the neoajuvant treatment phase received surgery.
Following erlotinib treatment, the response rate was 32% and the disease control rate was 76%; 16 patients were evaluated as resectable and underwent surgery. R0 resection was performed in 15 (93.8%) patients, which yielded a resection rate of 60%. The pCR was 6.3% and the pathological resection rate (pRR) was 93.7%.
Following surgery, patients received long-term follow-up including a quarterly chest CT scan for up to 2 years. The post-surgical median DFS (from operation) was 10.4 months. OS data are not yet mature.
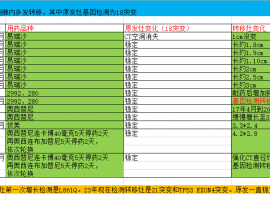
EGFR mutation status remained unchanged before and after the surgery in most patients with the exception of 3 patients with an exon 19 deletion that changed to EGFR wild type after resection.
There were a few adverse events following erlotinib treatment and most were mild; 7 (28%) patients had grade I rash and one (4%) patient had grade I diarrhoea. One patient with hepatitis comorbidity had grade IV abnormal liver function. One patient experienced a serious adverse event, cerebral infarction, with neoadjuvant erlotininb.
Dr Wilfried Eberhardt of the West German Cancer Centre in Essen, who discussed the results, said that the study authors presumed that induction therapy in EGFR mutation positive stage IIIA(N2) NSCLC patients is comparably effective for downstaging and downsizing as induction chemotherapy. Never smoker and women seem to have the most benefit from such an approach. However, PFS and DFS results are not convincing yet.
The majority of patients in this study did not receive the standard number of adjuvant chemotherapy cycles (n = 4). Therefore, a historical comparison to patient groups with surgery plus adjuvant chemotherapy is significantly hampered.
Dr Eberhardt expressed criticism that a restriction to common mutations and never smoker and women may be more suitable than to investigate such an approach in a curative setting unselectively. He questioned the best time and schedule of adjuvant/neoadjuvant chemotherapy in such setting that is currently unknown and said that chemotherapy is actually proven to be curative in this setting.
ConclusionsThe authors concluded that erlotinib as neoadjuvant therapy is a promising treatment for patients with EGFR mutant IIIA-N2 NSCLC that resulted in most patients being evaluated as resectable and elegible for surgical resection of tumours. The findings need to be further confirmed in a prospective phase III trial. Patients showed tolerable toxicity with neoadjuvant erlotinib with a serious adverse event occurring in just one patient.
Reference





 提升卡
提升卡 置顶卡
置顶卡 沉默卡
沉默卡 喧嚣卡
喧嚣卡 变色卡
变色卡 千斤顶
千斤顶 显身卡
显身卡